
 Background:Endotracheal intubation is a common occurrence in the ED. Many patients requiring airway management are at a higher risk of hypoxia due to deranged respiratory physiology (i.e. decreased functional residual capacity and/or increased shunt fraction). Advocates of video laryngoscopy argue that it provides better visualization of the airway anatomy, but it is less clear if better visualization correlates with better patient oriented outcomes. Good preparation, pre-oxygenation, and having a plan A, B, and C prior to intubation are essential requirements in 1st pass intubation success rate and decreased intubation time. What is less clear is should plan A be VL or DL?
Background:Endotracheal intubation is a common occurrence in the ED. Many patients requiring airway management are at a higher risk of hypoxia due to deranged respiratory physiology (i.e. decreased functional residual capacity and/or increased shunt fraction). Advocates of video laryngoscopy argue that it provides better visualization of the airway anatomy, but it is less clear if better visualization correlates with better patient oriented outcomes. Good preparation, pre-oxygenation, and having a plan A, B, and C prior to intubation are essential requirements in 1st pass intubation success rate and decreased intubation time. What is less clear is should plan A be VL or DL?
What They Did:
- Meta-analysis of randomized controlled trials evaluating video laryngoscopy (VL) vs direct laryngoscopy (DL) in adult patients in the emergency department undergoing endotracheal intubation
Outcomes:
- Primary: First pass intubation success rate (An intubation attempt began when the laryngoscope entered the mouth and ended when it was removed. An intubation attempt was considered successful when confirmed by capnography and additional standard techniques.)
-
Secondary:
- Overall intubation success rate
- In-hospital mortality
- Esophageal intubation rate
Inclusion:
- Randomized controlled trials
- Adult patients presenting to the ED
Exclusion:
- Trials on cadavers
- Trials on manikins
- Simulated reviews
- Non-English publications
Results:
- 1250 patients from 5 RCTs

Strengths:
- Included on only RCTs
- A number of databases were reviewed for appropriate articles (Cochrane, CENTRAL, etc…)
- Asks a clinically important question
- Followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)
- Cochrane questions were used to assess methodological quality of included studies
Limitations:
- The protocol for this meta-analysis was not registered
- There was no blinding of participants and personnel in the individual studies, potentially causing a performance bias
- All included studies were small
- There is a wide range of heterogeneity most likely due to differences in patients and operator expertise levels
- Incidence of hypoxemia was only reported in one trial and therefore not able to be evaluated in this meta-analysis
- Most of the included studies excluded patients with potentially difficult airways. It is this population where VL may have an advantage over DL.
Discussion:
- In the 5 trials included, 3 trials were a comparison of C-MAC VL vs the Macintosh blade and in the remaining 2 trials Glidescope VL vs the Macintosh blade were compared
- Potential reasons why VL was not superior to DL:
- Limited experience with VL
- RSI medications may not have been optimal during emergency intubation
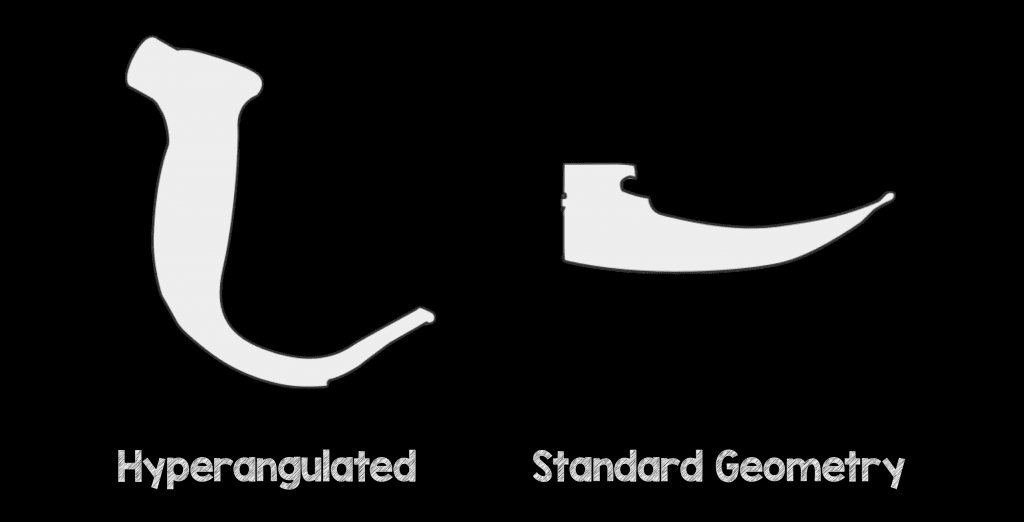
- VL may have had a poorer alignment of oral, pharyngeal and laryngeal axes (Not all VL is the same. There are hyperangulated blades as well as standard geometry blades)
- Finally, my thoughts on the VL vs DL debate are summarized in the image below
Author Conclusion: “Use of video laryngoscopy for emergency endotracheal intubation in adult patients is associated with reduced oesophageal intubation over direct laryngoscopy. However, no benefit was found in terms of overall intubation success.”
Clinical Take Home Point: Although there is no difference in 1st pass intubation rate, overall intubation rate, time to intubation, and in-hospital mortality, all of which are clinically important outcomes when comparing video laryngoscopy to direct laryngoscopy, better airway anatomy visualization with video laryngoscopy does reduce esophageal intubation rate compared to direct laryngoscopy.
References:
- Bhattacharjee S et al. A Comparison Between Video Laryngoscopy and Direct laryngoscopy for Endotracheal Intubation in the Emergency Department: A Meta-Analysis of Randomized Controlled Trials. J Clin Anesth 2018. PMID: 29549828
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami)
The post Video Laryngoscopy (VL) Or Direct Laryngoscopy (DL) in the ED appeared first on REBEL EM - Emergency Medicine Blog.